Open Access
Case report
Max Screen >>
ISSN: 2348-9820
Copyright: © 2015 Attia TH. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Kawasaki disease is an acute vasculitis of childhood. There is varying incidence among ethnic groups with higher rates among Asians.
An Egyptian male adolescent 12 years old presented with fever, loss of appetite, nausea and vomiting for 3 days. He had convulsion on admission. Physical examination revealed positive meningeal signs. Treatment of meningitis was started with no response. On day 6 of fever maculopapular skin rash appeared as well as bilateral non purulent conjunctivitis. Laboratory tests were in support for incomplete Kawasaki disease but Echocardiography was normal. Intravenous immunoglobulin and aspirin were started with marvelous response. On 12th day of fever, skin desquamation appeared mainly on perineal area and on tips of fingers and toes. The patient was classified as risk level I, and his family was advised for counseling every 5 years.
High index of suspicious is required for early diagnosis and management of Kawasaki disease irrespective of the clinical presentation or ethnicity. Early diagnosis can be a good prognostic index.
Keywords: Kawasaki disease; Meningitis; Egyptian; Intravenous immunoglobulin; Echocardiography
Kawasaki disease (KD) is an acute vasculitis of childhood that predominantly affects the coronary arteries. The etiology of Kawasaki disease remains unknown. A genetic predisposition is likely, based on varying incidence among ethnic groups, with higher rates among Asians [1].
Diagnosis of KD is based upon the presence of the characteristic fever, bilateral non exudative conjunctivitis, erythema of the lips and oral mucosa, rash, extremity changes, and cervical lymphadenopathy typically develop after a brief nonspecific prodrome of respiratory or gastrointestinal symptoms [2]. It occurs most often in babies and children, aged 6 months to 5 years [3]. Guidelines by the American Heart Association (AHA) and the American Academy of Pediatrics (AAP) were developed for the treatment of Kawasaki disease [4].
Kawasaki disease is very rare among Egyptian children. Review of literature revealed only 2 reported cases among Egyptian [5,6].
Here we are reporting a case of incomplete Kawasaki disease in an Egyptian adolescent who presented with meningitis which is not one of the classic criteria of Kawasaki disease. Echocardiography revealed no coronary aneurysm (CA). He was diagnosed early and successfully treated.
An Egyptian male adolescent 12 years old presented with high fever, loss of appetite, nausea and vomiting for 3 days. On admission, he had convulsion. Physical examination revealed neck stiffness, positive Brzezinski's and Kerning's signs which are positive meningeal signs. Chest, heart, abdomen, and musculoskeletal systems examination was normal. Complete septic work up was done including lumber puncture and cerebrospinal fluid (CSF) examination. Treatment of meningitis was started and fever did not respond. On day six of fever maculopapular skin rash appeared on the face, trunk and extremities and bilateral non purulent conjunctivitis. Laboratory findings upon admission, revealed leukocytosis with neutrophilia and shift to the left, anemia and normal platelets. Acute phase reactants were elevated. Serum creatinine, alkaline phosphatase, lactate dehydrogenase, creatine kinase, ferritin and bilirubin were normal. Aspartate transaminase (AST), Alanine transaminase (ALT) were high, while serum albumin was low. Urine analysis was normal. Results of blood, CSF, throat and urine bacterial cultures and serological tests for bacteria and viruses were negative. CSF result revealed WBC of 4 /mm3. CSF glucose was 65 mg/dl while blood glucose was 98 mg/dl and CSF protein was 22 mg/dl, the result which suggested aseptic meningitis. Viral screening from CSF was negative for herpes virus and enterovirus. Investigations performed had excluded the common causes with CNS involvements, including metabolic diseases, bacterial meningitis, tuberculosis, and viral infections. Encephalopathy in our patient could be considered as specifically related to Kawasaki disease. Based on clinical finding and laboratory results and after exclusion of possible other etiology KD was suspected and Echocardiography was done and it was normal. Intravenous immunoglobulin (IVIG) in a dose of 2 g/kg and aspirin 80 mg/kg orally were started and antibiotics were discontinued. Temperature subsided 24 hours after IVIG therapy and the child was very active. Thrombocytosis was evident from 8th day of fever. On 12th day of fever, skin desquamation appeared mainly on perineal area and on tips of fingers and toes (Figures 2-4). Follow up laboratory investigations were done with gradual normalization of acute phase reactant, CBC, ALT, AST and serum albumin (Figure 1). Low dose aspirin therapy 5 mg/kg per day, for its antiplatelet effect, was continued till normalization of acute phase reactants. Echocardiography was repeated twice with 6 months interval and it was normal. The patient was followed up for 3 years and he was in a good health with normal growth and development.
Diagnosis of KD is mainly clinical and the laboratory investigations may be valuable in the diagnosis of incomplete KD [7]. KD is suspected if an individual has persistent fever for more than 5 days which is not responding to broad-spectrum antibiotics and there is no proof of infection. Four out of the five following criteria must be present: i) polymorphous rash; ii) conjunctivitis; iii) cervical lymphadenopathy; iv) oral changes including injected pharynx or lips, cracked or fissured lips, strawberry tongue; v) extremity changes starting with edema or erythema and then progressing to desquamation of feet and hands, starting periungually [2]. Unfortunately, these diagnostic criteria are valid for the diagnosis of KD in children, but have not yet been validated in adults. About one-fourth of adult KD cases have occurred in patients with human immunodeficiency virus (HIV) infection [7]. One review found that cervical lymphadenopathy, hepatitis, and arthralgia were all more common in adults with KD than in children, and meningitis, thrombocytosis, and CA aneurysms were less common [8]. Splenomegaly and elevated serum ferritin levels were reported in one adult patient, most likely due to macrophage activation syndrome (MAS) complicating KD [9]. In Patients between 10 - 21 years old, ischemic heart disease developed in 4.7%, Myocardial infarction occurred in 1.9%, Bypass surgery was required in 1.2% and Overall mortality 0.8%. Age more than 10 years is a poor prognostic factor [10]. Our patient presented by fever for 3 days and on the day of admission he had meningeal signs. He received treatment for meningitis but with no response. On 6th day of fever he developed maculopapular skin rash and bilateral non purulent conjunctivitis. Our differential diagnosis covered a wide range of diseases, mainly infectious and autoimmune; none of them could be proved. There was no history suggestive of drug allergy. KD is diagnosed mainly by exclusion. Any fever more than 5 days with skin rash and without response to medication must give attention to possibility of incomplete KD, which need supportive positive laboratory finding. There was anemia, leukocytosis for the age as well as thrombocytosis. Meanwhile, ALT and AST were high and serum albumin was low. These positive laboratory criteria were in support for incomplete KD. Initial presentation of our case is meningitis, which is a rare presentation for KD. The pathogenesis of aseptic meningoencephalitis in KD is unclear. KD is characterized by systemic vasculitis, mainly involving the coronary arteries. Such a pathologic mechanism may also affect the CNS and be responsible for the neurologic symptoms. This was speculated to be the result of systemic vasculitis or the result of vascular leakage through the blood-brain barrier. A previous study with single-photon emission computed tomography imaging demonstrated localized cerebral hypo perfusion without neurologic findings. In another autopsied study, varying degrees of inflammatory changes in brain vasculature (leptomeningeal thickening, mild endarteritis, and periarteritis) was noted [11]. Husain and Hogue described an 11-year-old boy who presented with meningoencephalitis and was found later to have KD [12]. Madrigal et al. described two cases of aseptic meningitis over 6 years period among 23 patients who suffered from KD [13]. Muzaffer and Al-mayouf described three cases of aseptic meningitis over 5 years period among 13 patients who suffered from KD [14]. Incomplete KD should be suspected and laboratory evaluation performed in patients less than six months of age with unexplained fever ≥7 days, even if they have no clinical findings of KD, and in patients of any age with unexplained fever ≥5 days and only two or three clinical criteria [4]. In our case there was bilateral nonexudative conjunctivitis, which is present in more than 90 percent of patients [15]. There was no cervical lymphadenopathy, which is the least consistent feature of KD, absent in as many as one-half to three-quarters of children with the disease [16]. Mucositis which may occur singly, in a very mild form, or not at all [17]. In our patient skin desquamation appeared on 12th day of fever which add clinical support for diagnosis of KD. Extremity changes which is reported to vary from 98 to 68 percent [18]. IVIG was started immediately with marvelous response. The decision for use of IVIG was on clinical suspension for diagnosis of KD and supported by positive laboratory finding, and before appearance of skin desquamation. It is worth noting that even with adequate and timely administration, within ten days of IVIG and aspirin, 5% of patients develop coronary abnormalities [19]. Echocardiography was normal in our patient, and low dose aspirin was continued till normalization of acute phase reactants in the absence of coronary artery aneurysm [4]. Our patient was followed up for one year by Echocardiography with consistent normal finding. In the absence of coronary artery aneurysm, our patient was classified as risk level I, and his family was advised for counselling every 5 years [18].
High index of suspicious is important to diagnose Kawasaki disease in the acute phase. Early diagnosis and proper management are valuable in long term prognosis irrespective of the clinical presentation or ethnicity.
The authors have to acknowledge Dr. Hesham Fawzy assistant professor of clinical pathology who performed all laboratory tests for our patient.

![]()

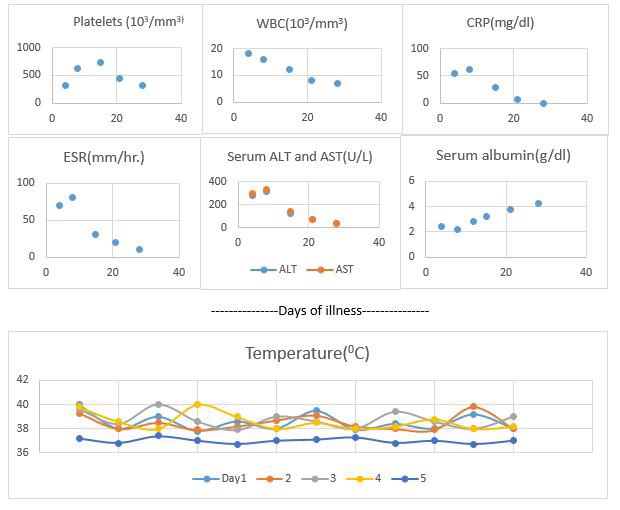 |
| Figure 1: Follow up of clinical course of fever and other laboratory results |
 |
| Figure 2: Skin desquamation of the perineum and thighs (in different positions) |
 |
| Figure 3: Skin desquamation of the thumb |
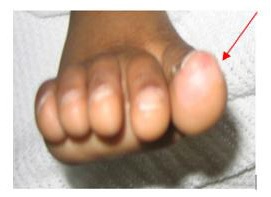 |
| Figure 4: Skin desquamation of the big toe |
|
| Figure 2: Skin desquamation of the perineum and thighs (in different positions) |
|
| Figure 3: Skin desquamation of the thumb |
|
| Figure 4: Skin desquamation of the big toe |












