Open Access
Case Report
Max Screen >>
ISSN: 2348-9820
Copyright: © 2015 Metgud R. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Dermoid cysts are uncommon clinicopathological lesions of developmental origin. Their etiology is not yet clear and can be associated with entrapment of ectodermal and mesodermal components when the 1st and 2nd branchial arches of each side fuse in the midline. The entrapped tissues then undergo proliferation and cystic transformation. These benign lesions are encountered throughout the body and rarely occur in the head and neck region, 1.6 to 7%. In this case, a 35 year - old- male presented with a painless swelling in the submental region at the right front side of neck. Although various investigations pinpoint to the diagnosis, the final confirmation is obtained after histopathological examination of the excised cyst and the present case was confirmed to be a dermoid cyst.
Keywords: Dermoid cyst; Submental region; Neck region
Dermoid cysts are cystic malformations that can arise in the head and neck area with an incidence ranging from 1.6% to 7% [1]. Of these, approximately 11.5% are located in the floor of the mouth which is the second most common location (lateral eyebrow being the most common) [2]. There is no sex predilection and the dermoid cysts are common affecting people between the ages of 15 and 35 years, during a period of maximal epithelial activity [1]. They are thought to be congenital in origin, by entrapment of pluripotent cells along the lines of embryonic fusion [3] but the literature also indicates they can also develop from acquired factors such as trauma or surgical implantation that forces epithelial cells into deep tissues [4].
The common midline cystic masses in the neck are thyroglossal cyst, thyroid cyst, sublingual dermoid cyst, suprasternal space abscess, subhyoid bursitis, ludwig’s angina. Dermoid cysts must be considered in the differential diagnosis of head and neck masses [5].
A 35 year old male patient presented with a painless swelling below the chin over the right front of the neck, which had been present for the past two months (Figure 1). There was a history of painless swelling initially which regressed in size after a course of antibiotics. He was moderately built with history of respiratory disease 15-20 years back. Family history was noncontributory. On inspection, spherical extra oral swelling was evident it submental region measuring 3x3.5 cm approximately. On palpation, swelling was soft to firm in consistency, non-tender on palpation, overlying skin was normal in color and temperature. Blood investigations revealed all levels within normal range. Lymph nodes were not palpable. A sonogram of submental region revealed subcutaneous swelling in the submental region more on right side. Since patient was not willing for surgical treatment, therefore advised to continue with the antibiotics and recalled after 5 days.
Patient revisited after 1 month with history of pus discharge 7- 8 days back. On inspection and palpation, swelling had regressed in size, ovoid in shape and non-tender on palpation. To rule out tuberculosis, PA CHEST view radiograph, microbiological examination like sputum for ACID FAST BACILLI and MONTOUX TEST were advised. Conventional radiographs, Chest x ray and AFB test were within normal limits (Figure 2,3 and 4). Montoux test was positive confirmed past infection with tubercle bacilli but it does not indicate presence of active stage of the disease. Based on the radiographs and FNAC a provisional diagnosis of epidermoid cyst or sebaceous cyst was rendered. The patient underwent surgery and the cystic lesion was totally removed (Figure 5).
Histopathologically, low power view revealed a cystic cavity lined by orthokeratinized stratified squamous epithelium and connective tissue stroma. Connective tissue stroma revealed skin appendages like hair follicle, sebaceous glands in the background of bundles of dense and diffuse collagen fibers interspersed with numerous fibroblasts with infiltrate of inflammatory cells and vascular spaces (Figure 6). The High Power view confirmed orthokeratinised squamous epithelium with connective tissue revealing skin appendages and mixed inflammatory cells chiefly lymphocytes and plasma cells, features suggestive of dermoid cyst.
The word “Dermoid cyst”, is a generic term which has been used to encompass and describe three different histological varieties: epidermoid (lined with simple squamous epithelium), dermoid (when skin adnexa are found in the cyst wall) or teratoid (when other tissues, such as muscle, cartilage and bone are present) [6,7]. The origin of dermoid cysts is thought to be congenital in most cases, but they also can be acquired [4,5].
Congenital: Origin from the embryonic cells of the first and second branchial arch entrapment during the third to fourth weeks of intrauterine life. Alternatively, may also crop up from the tuberculum impar of His, which forms the body of the tongue and floor of the mouth with each mandibular arch.
Acquired form: Due to epithelial cell implantation of the injury or surgery.
Clinically, the lesion presents as a slow-growing single, localized, mobile, soft, firm or doughy, usually well circumscribed, asymptomatic mass, usually located in the midline, above or below the mylohyoid muscle [6]. When located above the muscle, the cyst manifests itself as a sublingual swelling; when below the muscle, the clinical aspect will be a submental swelling [8]. Consequently, tongue elevation, speech alteration or double-chin development are frequent complaints. Because they are almost always asymptomatic, dermoid cysts are usually diagnosed only after they have reached a considerable size [7]. Histologically, dermoid cysts are lined by epidermis with the contents of keratinaceous, caseous, sebaceous, or purulent with hair, nails, fat globules, and even cartilage [6].
Recommended preoperative diagnosing techniques include ultrasound, CT scan, MRI, and fine needle aspiration biopsy. MRI is usually necessary to determine the exact location within the surround¬ing soft tissues as the cyst wall may tightly adhere with its sur¬roundings. Ultrasound is a reasonable initial imaging study as it is readily available, cost effective, and does not expose the patient to ionizing radiation, appear as solid and cystic structures within a heterogeneous Mass [4]. On CT scans, the dermoid cyst appear as moderately thin walled, unilocular masses filled with a homogeneous, hypoattenuating fluid substance with numerous hypoattenuating fat nodules giving the pathognomonic “sack-of marbles” appearance [9]. The specific histological type can be confirmed by histopathological examination, after excision.
Treatment is total extraction (enucleation) via the intraoral or extraoral approach or a combination of both. An intraoral approach is recommended in cases of cysts above the mylohyoid muscle and the extraoral technique is chosen in very large lesions which affect submandibular region and in situations of infection process that may interfere to patient’s airway[1]. Recurrence of dermoid cysts is not expected, and malignant transformation, though rare, has been reported in 5% cases [3,7].

![]()

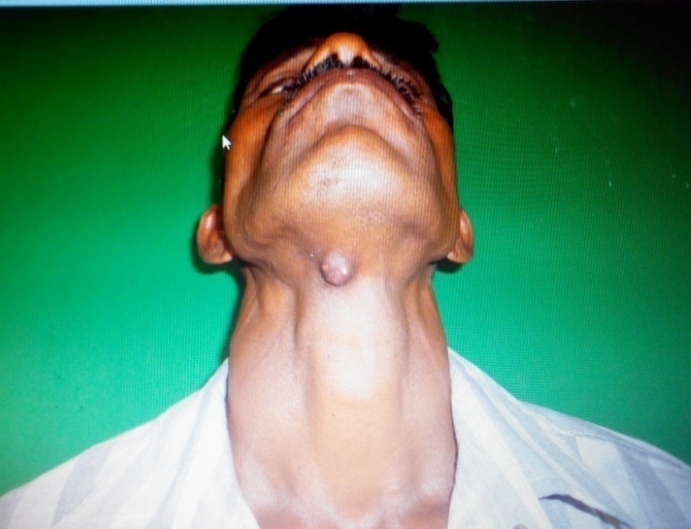 |
| Figure 1: Swelling below the chin |
 |
| Figure 2: Lateral neck view |
 |
| Figure 3: Occlusal radiograph |
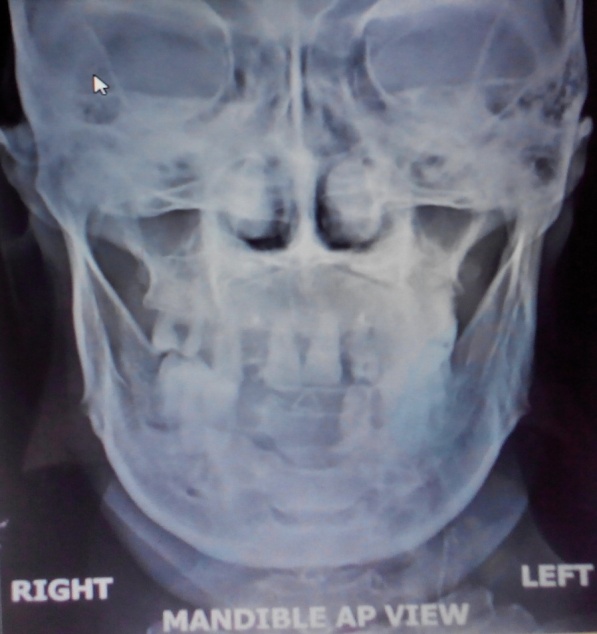 |
| Figure 4: Antero posterior mandible view |
 |
| Figure 5: Macroscopic view of enucleated lesion |
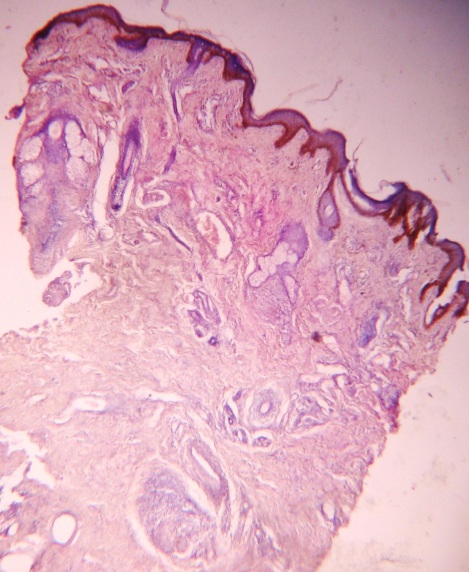  |
| Figure 6: Microscopically, a cystic cavity lined by orthokeratinized stratified squamous epithelium with cutaneous attachments, such as sebaceous glands and hair follicles (4x and 10x objective) |












