Open Access
Research Article
Max Screen >>
ISSN: 2641-7847
Copyright: © 2018 Cubillana-Herrero JD. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Related article at Pubmed, Google Scholar
Background: We have analyzed the effect of the learning curve on the implementation of the Cochlear Implant Program in terms of intra and postoperative results. Here we present the results and complications found in our series, as well as what we believe is the most interesting aspect, the learning curves for two variables: complications and mean hospital stay.
Methods: The series consisted of 64 patients, all of which underwent a cochlear implantation between January 2003 and December 2010. The patients in the series were included in the cochlear implantation program at the Hospital Clínico Universitario Virgen de La Arrixaca (HCUVA) with a diagnosis of hypoacusia identified in newborn screening or using other means. The device was recommended in people with bilateral neurosensorial hypoacusia of cochlear origin or those who had not benefited from, or only slightly benefited from, the use of hearing aids. Our group used the indications for cochlear implants of the Federal Food and Drug Administration (FDA).
Results: Thirty-two of the cases were females (50%). Their mean age was 5.56 years with an age range of 1-64 years and a mode of 5 years (15.6%), with 51.6% cases being below 6 years of age, and 75% were younger than 11 years. The family’s cultural awareness level was low in 19 cases (29.7%), average in 33 (51.6%) and high in 12 (18.8%). 87.5% of cases (56 cases) did not have any postsurgical complications, with this occurring in only 8 cases (13.5%): 4 cases of skin dehiscence (6.3%), 1 cerebrospinal fluid (CSF) leak (1.6%), 1 skin necrosis (1.6%), 1 hemorrhage (1.6%) and 1 case of postoperative seroma.
Conclusion: Our results can be compared with those of other national and international hospitals and do not compromise patient safety.
Keywords: deafness; infants; cochlear implants
Deafness is defined as a deficiency and refers to the loss or abnormality of an anatomical and/or physical function of the hearing system, and as an immediate consequence there is an immediate hearing disability, which means that there is a deficiency in the patient’s access to oral language [1]. Currently, the disability is understood as a dynamic situation and not a stable quality, which varies in each individual according to his or her interaction with his or her surroundings. Following along these lines, it is possible to understand that a deficiency will bring about limitations in daily activities and restrictions in the social participation to a varying degree depending on who has it [1]. Furthermore, the perception about the subject’s own quality of life will be different at the same levels of deficiency.
It has been calculated that the annual incidence of hypoacusia is five cases per thousand newborns, of which one in each thousand presents at birth with severe or profound deafness. Around two thousand families will be affected each year by the presence of a hearing impairment in one of their children. It is of great importance that 80% of cases of deafness are present at birth, that 60% of child deafness cases have a genetic origin and that in only 50% of newborns with deafness is it possible to identify developmental risk factors [2,3].
We have analyzed how the influence of the learning curve in the introduction of a cochlear implant program on intra and postoperative results. We present the results and complications in our series as well as what we believe to be the most interesting aspect: the learning curves for the variables of complications and mean hospital stay.
The series consists of 64 patients, all of whom underwent a cochlear implant between January 2003 and December 2010. The patients in the series were in included in the cochlear implant program of the Hospital Clinico Universitario Virgen de la Arrixaca (HCUVA) with the diagnosis of hypoacusia thanks to its identification in newborn screening or by other methods.
The device was recommended in people with deep bilateral neurosensorial hypoacusia of a cochlear origin who received no or hardly any benefit with the use of hearing aids. Our group used the indications for cochlear implants of the Federal Food and Drug Administration (FDA).
50% (32 cases) were implanted between 2003 and 2007, while the other 50%, the 32 remaining cases, were implanted between 2008 and 2010. The mean number of implants per year were 8 cases with a range of 2-11 cases/year. The cochlear implant was carried out in the right ear in 49 cases (76.6%), while in 15 patients (23.4%) the implant was in the left ear.
Microsoft Excel version 2010 (Redmond, Washington, USA) was used for data entry, and SPSS (IBM Corp.; version 21, New York, USA) software was used for data analysis.
Approval was obtained from the ethical approval committee of the HCUVA, and the testing was done using non-invasive procedures. The objectives and procedures of the study were explained to the participants before evaluation, and informed consent was obtained prior to participation.
We consider a learning curve as the necessary interventions to make statiscally significant the variables (hospital stay and complications) into cochlear implant program
Of all the cases 64 were females (50%). The mean age was 5.56 years with an age range of 1-64 years and a mode of 5 years (15.6%), with 51.6% of the cases being under 6 years of age and 75% under 11 years. The cultural awareness level of the families was low in19 cases (29.7%), average in 33 (51.6%) and high in 12 (18.8%).
There were family antecedents of interest regarding deafness in only 8 cases (12.5%); specifically, 6 cases (9.4%) had antecedents of family deafness, and in 2 cases (3.1%) one of the subject’s ancestors had been diagnosed with Chagas disease. The comorbidity that was associated in 46 cases (71.9%) did not have any antecedent of interest regarding the deafness that the patient suffered from. In 18 cases there were antecedents of interest: 5 cases (7.8%) of prematurity, 4 cases (6.3%) of neonatal encephalopathies, 2 cases (3.1%) of meningitis and 2 cases (3.1%) of associated syndromes (1 Goldenhar syndrome and another of an unknown cause). The distribution of the patients of the series and their personal antecedents are shown in Table 1.
Thirteen cases (20.3%) presented with auditory surgical transtympanic drainage prior to cochlear implant. The remaining 51 cases (70.7%) had not been given any previous hearing surgery.
With regard to the audiometry tests that were carried out in 100% of the patients, these demonstrated the presence of bilateral anacusis in 50 cases. (78.1%). In 12 cases (18.8%) the audiometry revealed a positive response of between 80 and 100 decibels (dB), while in only 2 cases, (only 3.1%), that response was below 80dB.
The spontaneous acoustic otoemissions at birth, carried out in 35 cases (54.7%), were only present in 4 cases (14.2%) and absent in the remaining 30 (85.7%). Brainstem evoked response audiometries (BERA) were performed in all the cases, demonstrating the presence of anacusis in 44 cases (68.8%), the presence of a response of between 80-100dB in 18 cases (28.1%), and a response of at least 80dB in 2 cases (3.1%). The tympanogram, which was also performed in all the cases, was normal in 51 cases (79.7%) and flat in 13 cases (20.3%).
With regard to the anatomical tests, all the patients in the series were given a Computed Tomography (CT) and Nuclear Magnetic Resonance (NMR), demonstrating the presence of a narrowing of the channels in 2 cases (3.1%) and calcification of the inner ear in a further 2 cases (3.1%). The remaining 60 cases (9.8%) presented a normal hearing anatomy.
The mean waiting time during which the patients were assessed in the consultation was 57.53+3.39 days, with 50% of the cases having mean times of less than 52 days and 75% had less than 78 days, with a mode of 36 days (14.1%). Once the case was accepted for an implant, the mean time from its inclusion on the waiting list until the implantation was 49.89+3.64 days. 50% of the cases waited less than 46 days and 75% less than 72 days, with a mode of 48 days (12.5%).
The mean hospital stay was 5.56 days with a range of 2-9 days and a mode of 5 days (20 cases, 20.3%). 51.6% of the cases had a stay of less than 5 days and 90% of less than a week.
We did not have any intraoperative complications.87.5% of the cases (56 cases) did not present with any postsurgical complications; these were only found in 8 cases (13.5%): 4 cases of skin dehiscence (6.3%), 1 of lateral semicircular canel (LSCC) fistula (1.6%), 1 skin necrosis (1.6%), 1 hemorrhage (1.6%) and 1 case of postoperative seroma (1.6%). The complications of the series are recorded in Table 2.
It is notable that on 3 occasions it was necessary to remove the implant and to proceed, a posteriori, to cochlear reimplantation: in 2 cases this was due to a failure in the electrode not associated with any surgical complication, and in 1 case it was associated with skin necrosis.
Regarding the functional results, based on the audiometries carried out postoperatively, we will classify them according to frequencies. At the 250 Hertz (Hz) level, 87.5% of the cases had a hearing threshold of 35dB, with a mean of 29.5dB and a mode of 25dB (14 cases, 21.9%). At 500Hz, 89.3% had a threshold of 40dB, with a mean of 32.2dB and a mode of 30dB (17 cases, 26.6%). At 1000Hz, 91.1% of the cases could hear at 45dB, with a mean of 35.5dB and a mode of 30dB (15 cases, 23.4%). At 2000Hz, 91.1% could hear at 45 dB, with a mean of 33.4dB and a mode of 25dB (17 cases, 26.6%). Finally, at 4000Hz, 91.1% had a hearing level of 40dB, with a mean of 32.2dB and a mode of 25dB (17 cases, 26.6%).
One of the key objectives of the present study was to determine at which point the experience of the team is manifested in terms of the results, that is, after what number of interventions is there a statistically significant reduction in both hospital stay and the presence of complications. A comparison was made between the percentage values of both variables as well as the mean values of the hospital stay for 4 cut-off points established at 20, 25, 30 and 35 interventions.
As seen in Table 3 and in Figure 1, for a cut-off point of 20 interventions, statistically significant differences were found in terms of postoperative surgical complications. For instance, in the group of <20 interventions complications were observed in 30% of cases, compared to 4.5% in the group of >20 interventions (p=0.009). With regard to hospital stay, in the group of <20 cases, the percentage of cases with stays of >5 days was 60%, with a mean stay of 6.15+1.59, compared to 43.2% and a mean stay of 5.3+1.6 days in the group of >20 interventions.
Finally, for the cut-off point of 35 interventions the following results were found: in the group of <35 interventions, complications were found in 17.1% of cases, compared to 6.9% in the group of >35 interventions. Regarding hospital stay, in the group of <35 cases, the percentage of cases with stays >5 days was 60%, with a mean stay of 5.8+1.54, compared to 34.5% and a mean stay of 5.24+1.7 days in the group of >35 interventions (p=0.037).Table 4 and Figure 2.
When we consider these cut-off points in terms of the precise or necessary time to achieve them we see that 2.5 years were required to achieve 20 interventions; while in order to achieve 35 interventions, 4.3 years were needed. In other words, the learning curve had been overcome, taking into account a mean of 8 cases per year, after 2.5 years, in terms of complications; and after 4.3 years, in the case of hospital stay.
The objectives of a cochlear implant (CI) program include: adequately selecting the patients who are candidates for this kind of surgery; carrying out a safe and efficient implantation; and checking the patient’s subsequent progress with the implant to obtain the best functional results possible [4,5]. In our opinion, and based on the experience acquired using these first implants, in order to bring about an efficient treatment of profound hypoacusia through a CI program, the following action needs to be taken [4]. To introduce a program for the early diagnosis of hypoacusia, to allow for early cochlear implants so that better results can be obtained. We understand that the basis for the subsequent development of a good program of implants requires the creation of a Newborn Hearing Screening Program covering 100% of the newborns in our region. To form a multidisciplinary team to bring together the best professionals in each of our fields of interest, within our local region; and who, furthermore, are the most appropriate in terms of their professional capacities. In other words, we need to create a cochlear implant unit. To improve theoretical capacities by studying and learning the techniques and methods of cochlear implantation from the best schools and services in our country. To enable our patients, children and adults, after having received the implant, to obtain the best functional result, and in order to do this, adequate hearing rehabilitation should be organized in adults and this should be fully integrated and comprehensive in children. The problem of the location of the CI unit depends on the size of the Autonomous Community of the Region in which it lies; the number of hospitals in this region; and the distribution of the personnel and the resources available to them [4,5]. We have to take into account that in those Regions of a certain size, there are usually different hospitals in which appropriate multidisciplinary teams can be organized both at a diagnostic and therapeutic level and that these also attend to a sufficient number of cases. In addition, in the Autonomous Community Regions with smaller populations, the best professionals often work in several hospitals. However, given the lower number of patients to be assessed and therefore, the fewer candidates, it means that in order to maintain the right amount of quality, it would be better is they always operated in just one hospital. Consequently, to achieve the aforementioned objectives, especially in these small regions, effective inter-hospital cooperation will be necessary to achieve the best use of the healthcare resources available. In our case, an Autonomous Community Region with just one province with around one and a half million inhabitants, the implant program has been set up exclusively by the HCUVA. Our initial intention was to attend to patients in our study area and with the resources available to our hospital. In fact, we successfully carried out the first cochlear implant in the year of 2003.
When we consider volume of work, the number of implants should be enough to warrant the formation of an adequate team [4]. Acording to the literature review consider that there must be a minimum of 12 cases per year [3]. In this way it is hoped that an optimum use of resources will be achieved, and the capacities of the professionals will be guaranteed in this field where there are constant changes such as in the case of cochlear implants. In our particular case, in the Autonomous Community of the Region of Murcia, with a population of more than 1,500,000 inhabitants and approximately 10,000 annual births, the number of annual implants could be from about 6 to 8 children and approximately 15 to 20 adults, sufficient demand for a stable program of implants, with the necessary condition that the surgery be carried out in the same hospital and by the same surgeons. The program of cochlear implants in Murcia, therefore has a high enough number of participants to justify its existence.
Apart from these aspects, we believe that it would be essential to establish a series of policies for the creation of the program. In the first stage, and in order for the program to run more efficiently, we believe it would be a priority to introduce the program for children with early onset hypoacusia. It is for this reason that we have supported and participated in the policy of the early diagnosis of hypoacusia that was initiated, under the control of the Ministry of Health, by several Autonomous Community Regions. At a later stage, we designed diagnostic and therapeutic protocols adapted to our study area.
As a final consideration, the corresponding healthcare authority should be the organization to facilitate the implementation of the program providing the appropriate resources that should be adapted to the demand of the population so that homogeneous and adequate treatment can be provided to patients. In this regard, perhaps an interesting possibility could be the creation of a network of cochlear implant hospitals with a greater amount of experience and which is more highly qualified in this matter could become units of reference both for the candidates and the users of cochlear implants.
In all cases we have used the classic approach, the most widely used and accepted one, the one which uses the facial recess (FR) for passing the electrode from the mastoidectomy to the middle ear [5-10]. This technique requires a simple mastoidectomy and a posterior tympanotomy. At this point, the access to the middle ear is narrow and requires precision and experience from the surgeon, given that the presence of the facial nerve means that certain risks should be assumed. The opponents of this technique place considerable emphasis on this point, arguing that this access can be omitted, avoiding the proximity of the facial nerve and its possible complications.
Regardless of the design or means of the approach used, the dermal flap should be handled carefully and kept damp during the whole procedure. Whenever it is necessary to narrow the subcutaneous tissue, it is convenient to expose the flat surface of the pillous follicles, given that it can present with skin necrosis. Similarly, the edges of the incision should be designed in such a way as to be separated by at least 1.5-2.0cm from the receptor-stimulator (R/S), which should not interfere with or enter into contact with the microphone of the retroauricular processor in some of the current models.
With the use of traditional systems for inserting electrodes it was considered that intraocular injuries could be caused that might eliminate residual hearing [11]. For this reason, and in recent years, we have seen a paradigmatic change in the way the electrodes are introduced so that it has become the least traumatic possible through the use of specially designed and minimally-traumatic electrodes; and so-called soft surgery [12]. It is believed that there are at least three mechanisms responsible for intraocular mechanical damage during the insertion of the electrodes: spiral bone layer fracture or spiral ligament, something that normally occurs when the electrodes are inserted through the round window due to its proximity to this layer; a lesion of the lateral scale structures in the first basal turn of the cochlea; and due to the deep insertion of the electrode given that the greater the depth the narrower the turn radius and the smaller the section diameter [12-14]. The reduction in the damage associated with the insertion of the electrodes is based on the use of shorter and thinner electrodes with shallower insertion angles [14,15]. An electrode with these characteristics is less likely to cause damage when it comes into contact with structures of the cochlea; however, the greater the depth of the insertion, the more likely it is that surviving nerve fibers will be stimulated and there will be a better and wider dynamic range of hearing frequencies. The immediate question is: what is the ideal depth?; and what makes an insertion too deep? The studies available have confirmed that an insertion of only 6mm would allow for an excellent preservation of residual hearing but with a very poor gain in hearing which is estimated to be only 10% [16]. However, with electrodes of 10mm this gain would reach 40% [16]. If we want to stimulate low frequencies, the electrode should be inserted by nearly 500 degrees, one and a half turns, and with the design of current devices this would generate an unjustifiable amount of trauma [17].
After what number of interventions do the rates of complications and hospital stay come down in statistically significant way? With regard to complications, our analysis has revealed that after the first 20 surgical interventions when the number of complications falls drastically from 30% to 4.5%. Regarding stay, it is only after the thirty-fifth intervention when we observe a statistically significant percentage decrease, going from 60% of patients with hospital stays of more than five days (a mean stay of 5.8 days) to 34%, with a mean stay of 5.2 days in the group with more than 35 interventions. One question that immediately arises is the reason for the complications, after having reduced after the twentieth intervention, hospital stay does not do this at the same time but much later, after the thirty-fifth intervention to be exact. We believe that the reason for this is to be found in the fact that we are dealing with a surgical group in its initial stage of gaining experience. In this situation, and even after confirming a significant reduction in complications, the team is still not aware of this fact and thus cannot encourage an early discharge. It is only after the thirty-fifth intervention when it has been confirmed and assumed that this reduction in complications is firm and constant, that the mean stay has been reduced significantly.
Our results can be contrasted with other national and international hospitals, without compromising patient safety. The choice of the surgical technique is another piece of data about the experience of the members of the team and above all about its leader, although as reported in the results and discussion, the safest technique with the least number of complications has always been chosen.
Regarding the learning curve it is essential to follow other lines of research to confirm in other groups that a minimum number of interventions are needed to significantly reduce the percentage of complications and other variables that could be interesting for implementing in cochlear implant teams.
Ethics committee approval was received for this study from the ethics committee of Hospital Clinico Universitario Virgen de la Arrixaca. Murcia, Spain.
Informed consent was obtained from who participated in this study.
Concept JD; Design JP; Supervision JP; Resources JA; Materials AN; Data Collection and/or Processing MJ; Analysis and/or Interpretation MJ; Literature Search JD, JP; Writing Manuscript JD; Critical Review JP.
No conflict of interest was declared by the authors.

![]()

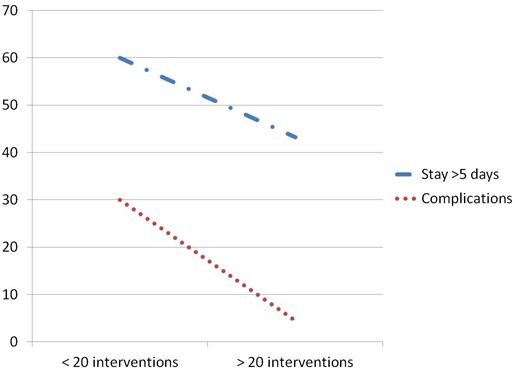 |
| Figure 1: Changes observed in stay and complications for interventions > or < than a number of 20 interventions. (Data in percentage terms) |
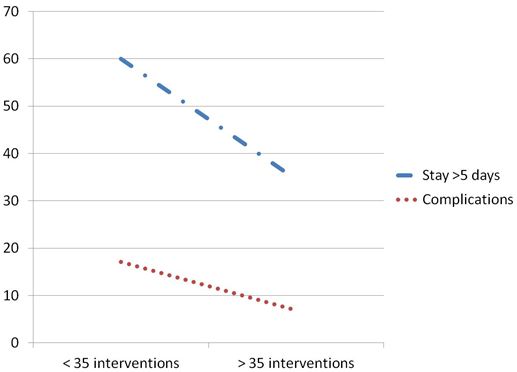 |
| Figure 2: Changes observed in stay and complications for the interventions > or < than a number of 35. (Data in percentage terms) |
| N | % | |
None |
46 |
71.9 |
Prematurity |
5 |
7.8 |
Meningitis |
2 |
3.1 |
Encephalopahy. Psychomotor retardation. Autism |
4 |
6.3 |
Plagiocephaly |
1 |
1.6 |
severe hearing loss |
1 |
1.6 |
TORCH infections |
1 |
1.6 |
Hypo/hyperthyroidism |
1 |
1.6 |
Genetic syndrome |
2 |
3.1 |
Chagas disease |
1 |
1.6 |
Total |
64 |
100 |
| TORCH: Toxoplasmosis, Other (syphilis, varicella-zoster, parvovirus B19), Rubella, Cytomegalovirus (CMV), and Herpes infections Table 1: Personal antecedents of the patients of the series |
||
| N | % | |
None |
56 |
87.5 |
Skin dehiscence |
4 |
6.3 |
Fistula LSCC |
1 |
1.6 |
Skin necrosis |
1 |
1.6 |
Hemorrhage |
1 |
1.6 |
Seroma |
1 |
1.6 |
Total |
64 |
100 |
| LSCC: lateral semicircular canal
Table 2: Postsurgical complications |
||
| P | |||
<20 |
70 |
30 |
0.009 |
>20 |
95.5 |
4.5 |
|
<25 |
76 |
24 |
0.034 |
>25 |
94.9 |
5.1 |
|
<30 |
80 |
20 |
0.092 |
>30 |
94.1 |
5.9 |
|
<35 |
82.9 |
17.1 |
0.198 |
>35 |
93.1 |
6.9 |
|
| p< 0,05 was considered significant
Table 3: Percentage results for the variable of postoperative surgical complications at 4 cut-off points established in 20, 25, 30 and 35 interventions. The statistically significant values are shown in red |
|||
P |
|||
<20 |
40 |
60 |
0.283 |
>20 |
56.8 |
43.2 |
|
<25 |
40 |
60 |
0.11 |
>25 |
59 |
41 |
|
<30 |
40 |
60 |
0.068 |
>30 |
61.8 |
38.2 |
|
<35 |
40 |
60 |
0.037 |
>35 |
65.5 |
34.5 |
|
| p< 0,05 was considered significan
Table 4: Percentage results for the variables of hospital stay at 4 cut-off points established as 20, 25, 30 and 35 interventions. Statistically significant values are in red |
|||












